The WHO has posted video of its final meeting on the Pandemic Treaty. Basically there was formal approval of the draft, then every delegate who wished made concluding statements.
While they came up with a document, the negotiators do not look especially happy about it. They acknowledge this is only the “start” of pandemic preparedness.
Here is the final treaty draft:
Earlier versions used the word “shall” often, which meant that nations must obey those paragraphs beginning with “shall.” Most of those paragraphs are gone. When shall is used, it generally is modified by saying that domestic law will be taken into account, and/or subject to local conditions and resources—in other words, it does not bind nations, at this point. So although the delegates hammer the fact that this is a “legally binding” treaty, it really is not.
On page 1, the Biological Weapons Convention of 1972 is acknowledged. I did not see this nod to the existing, most relevant treaty in versions up to late 2024, when I last carefully reviewed a draft. It is an important addition, as it is about controlling research, production and proliferation of biological weapons—something earlier versions failed to do. And I would say they encouraged such research (in one draft suggesting GOF research should be managed by experts appointed by the WHO D-G) and their PABS program encouraged proliferation.
The issue of giving up sovereignty for health naturally touched a nerve for many nations. So at the bottom of page 1 is the following sovereignty guarantee, except coupled with “obligations under international law” providing a future opportunity to say international law trumps national law:
9. …respecting States’ rights to implement health measures in accordance with their relevant national law and obligations under international law, and recalling World Health Assembly Decision SSA2(5),
Unsurprisingly, governments all go along with censoring citizens:
15. Recognizing the importance of building trust and ensuring the timely sharing of information to prevent misinformation, disinformation and stigmatization,
The language now includes climate change, which could be a justification for declaring an emergency:
19. Recognizing the importance and public health impact of growing threats such as climate change, poverty and hunger, fragile and vulnerable settings, weak primary health care and the spread of antimicrobial resistance,
And while this draft restricts pandemics and “public health emergencies of international concern” to infectious diseases, it also defines a public health risk that could include climate change, gun violence, etc. (Article 1):
(h) “public health risk” means a likelihood of an event that may affect adversely the health of human populations, with an emphasis on one which may spread internationally or may present a serious and direct danger;
Now there is a lot being stated in the document about surveillance, risk assessment, strengthened immunization programs, etc., but without any specific requirements imposed on member states. It looks to me as if a number of goals are listed that at this time are voluntary, but the hope is to make them obligatory in future.
The Conference of Parties will be formed and will address all the difficult questions that could not be resolved in this document. (Article 4):
5. The Conference of the Parties shall develop and adopt guidelines, recommendations and other non-binding measures as necessary, to promote the effective implementation of the provisions set out in paragraphs 1 and 2 of this Article, consistent with the provisions of the IHR, following, as appropriate, a One Health approach, with full consideration of the national circumstances and the different capacities and capabilities of Parties, as well as the need for capacity building and implementation support for developing country Parties.
6. The Conference of the Parties, through its work in relation to the provisions of this Article, shall address, inter alia, cooperation for implementation, in particular through technical assistance, capacity building, research collaboration, facilitating equitable access to relevant products and tools, technology transfer as mutually agreed,* and financing in line with the provisions of this agreement; and cooperation to support global, regional and national initiatives aimed at preventing public health emergencies of international concern including pandemic emergencies, with particular consideration given to developing country Parties.
* Footnote: For the purposes of this agreement, “as mutually agreed” means willingly undertaken and on mutually agreed terms, without prejudice to the rights and obligations of the Parties under other international agreements.
For the life of me, I don’t understand how that footnote changed the meaning of the document so everyone would go along.
Article 5 (One Health) still says nations will promote the One Health approach.
Article 6 says nations will endeavor to have interoperable health information systems—in other words, no confidentiality.
Article 7 (4) has the same contradiction I pointed out earlier: minimize the brain drain of health professionals, while at the same time respecting their freedom of movement.
Article 9 (5) tells nations to develop policies that will allow EUA-type products to be used, with “promote timely and equitable access to such products” meaning “pandemic-related health products.” Timely being the word of concern.
Article 12 says that the Particles will establish a Pathogen Access and Benefit Sharing System (PABS system) and all the details will be agreed in a separate instrument of the future. At least now the document throws a bone to the issues of proliferation and lab leaks:
5(e) implementation consistent with applicable international law and with applicable national and domestic law, regulations and standards related to risk assessment, biosafety, biosecurity and export control of pathogens, and data protection;
and a promise of at least 10% but “targeting” up to 20% of medical products will be given free to WHO during a pandemic by “participating manufacturers” who have yet to be defined in the PABS document. This one paragraph is binding—but its provisions will be worked out in future! All the earlier paragraphs were not.
In Article 13, the old global supply chain network is established and to be convened by WHO, under the Conference of Parties (COP). The Parties shall allocate the goods. Who? How? The COP will figure this out later. I cannot imagine how the parties will agree on this matter going forward, when they only got this far after 3.5 years of intense negotiations.
Article 14 is where “Regulatory Strengthening” is inverted to mean regulatory weakening, as in earlier drafts:
2. Each Party shall take steps towards ensuring that it has the technical capacity, and legal, administrative, and financial frameworks, as appropriate, in support of: (a) expedited regulatory review and/or emergency regulatory authorization, and oversight of pandemic-related health products, consistent with applicable law;
Expedited being the operative word. Expedited authorization (approval) and oversight (of safety)—just what the doctor ordered. NOT. This IS BINDING—nations must at least “take steps” toward weakening regulation of pandemic products.
Article 17 talks about the pre-, post- and inter-pandemic periods, just so everyone knows a pandemic is just around the corner, and we should apply a pandemic ruler to periods of time, going forward. Keep engaging the community regarding pandemics so it will have a resilient response. But they never tell you what a resilient response to a pandemic might look like. Or how it can be created.Article 18 is the “trust the science” section:
2. Each Party shall, as appropriate, conduct research and inform policies on factors that hinder or strengthen adherence to public health and social measures in a pandemic and trust in science and public health institutions, authorities and agencies.
Article 20 is “Sustainable financing.” Where will the money come from to do anything? Leave it to the COP.
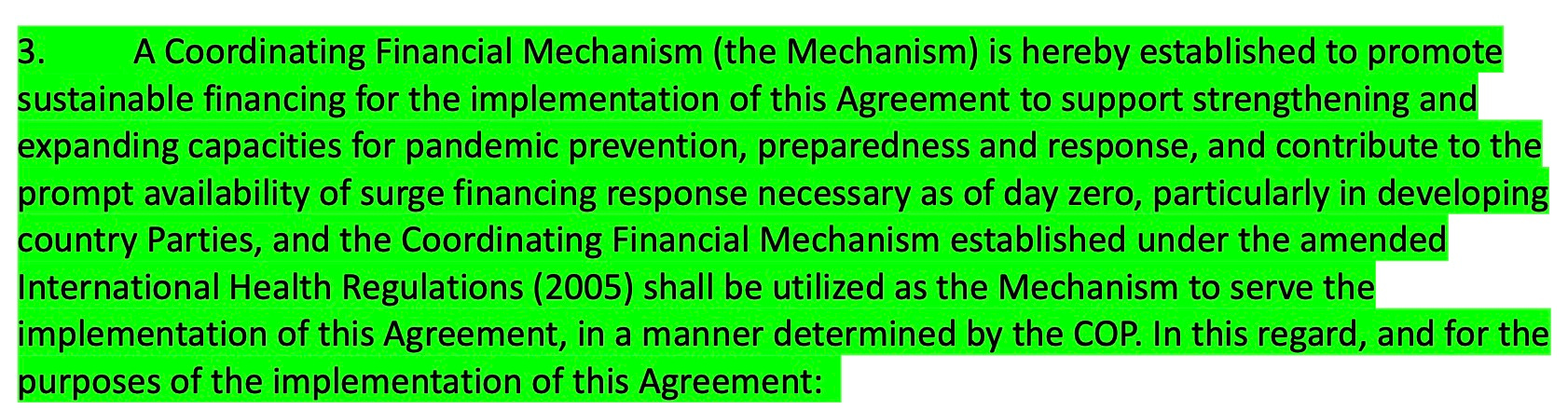
But if I understand this correctly, the COP mechanism is to make non-binding recommendations:

Article 24 asserts national sovereignty and tells the WHO and its D-G that it may not impose any requirements on states parties! And just to put a fine point on it, there will be no WHO-ordered vaccine mandates, tests, treatments or lockdowns!
Article 27 allows nations to make reservations (disagreements) with parts of the treaty. If I recall correctly, this was not permitted in earlier versions.
BOTTOM LINE:
This version of the treaty does not commit any nation to doing anything it does not want to do.
Nor does it promise nations anything of value: no privileges or benefits.
You might be lucky and get some free or cheap vaccine or drugs if manufacturers agree in future to give them away.
All the controversial areas have been kicked down the road.
There is nothing binding in this document that is a problem for nations.
If this was the level of agreement at 3.5 years, we can assume they won’t get much further over the next few years. The US and Argentina will be out. I imagine all the nations will approve this document, since it is virtually meaningless, only providing a skeleton —which the globalists hope can be dressed up later with the awful provisions. But since the globalists just had their biggest funding stream turned off (USAID) they made no obvious attempt to use bribery to gain agreement on more restrictive provisions. And even this meager document required an extra negotiating day and meetings to the wee hours.
Never say never, but I am very relieved. The Pandemic Treaty negotiations and what they finally drafted were "a tale told by an idiot, full of sound and fury. Signifying nothing."