https://www.medrxiv.org/content/10.1101/2023.06.09.23290893v1.full.pdf
ABSTRACT
Background. The CDC recently defined being “up-to-date” on COVID-19 vaccination as having received at least one dose of a COVID-19 bivalent vaccine. The purpose of this study was to compare therisk of COVID-19 among those “up-to-date” and “not up-to-date” on COVID-19 vaccination.
Methods. Employees of Cleveland Clinic in employment when the COVID-19 bivalent vaccine first became available, and still employed when the XBB lineages became dominant, were included. Cumulative incidence of COVID-19 since the XBB lineages became dominant was compared across the ”up-to-date” and “not up-to-date” states, by treating COVID-19 bivalent vaccination as a time-dependent covariate whose value changed on receipt of the vaccine. Risk of COVID-19 by vaccination status was also compared using multivariable Cox proportional hazards regression adjusting for propensity to get tested for COVID-19, age, sex, and phase of most recent prior SARS-CoV-2 infection.
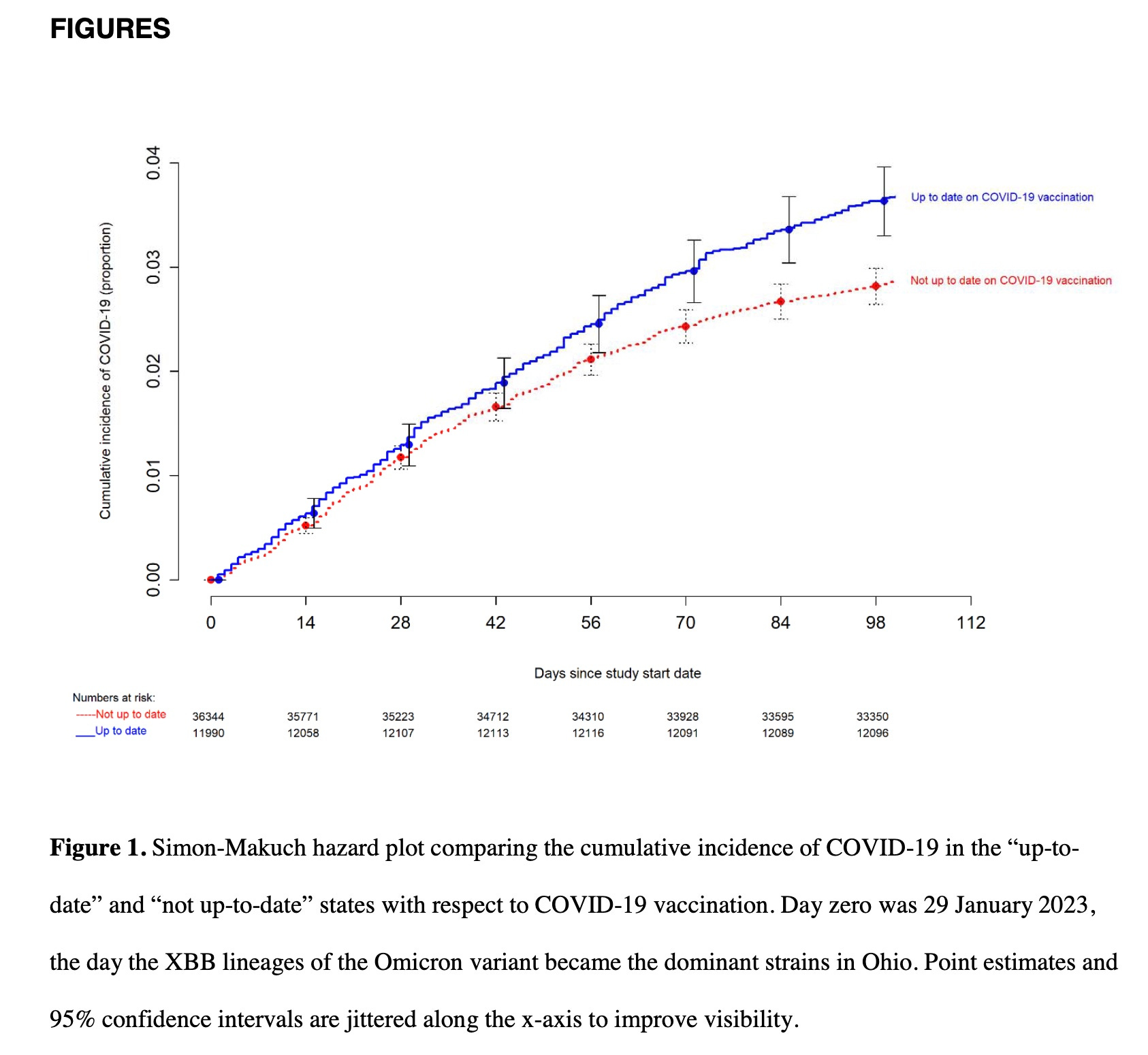
Results. COVID-19 occurred in 1475 (3%) of 48 344 employees during the 100-day study period. The cumulative incidence of COVID-19 was lower in the “not up-to-date” than in the “up-to-date” state. On multivariable analysis, not being “up-to-date” with COVID-19 vaccination was associated with lower risk of COVID-19 (HR, 0.77; 95% C.I., 0.69-0.86; P-value, <0.001). Results were very similar when those 65 years and older were only considered “up-to-date” after receiving 2 doses of the bivalent vaccine.
Conclusions. Since the XBB lineages became dominant, adults “not up-to-date” by the CDC definition have a lower risk of COVID-19 than those “up-to-date” on COVID-19 vaccination, bringing into question the value of this risk classification definition
You have to read between the lines to get it—or look at the graphs. The value of the risk definition is admittedly zero, but that is because the benefit of the vaccine is negative.
Cleveland Clinic has 50,000 employees and virtually all were vaccinated and masked for years. Only some are boosted. Only half have had symptomatic, diagnosed COVID. Articles like this have come out from time to time looking at this population of healthcare workers (probably the majority are nurses) to compare vaccine status with likelihood of infection.
The graphs are very important because the trends are consistent over time and between groups. You can also assume that epidemiologists have been all over these data, trying to make the findings go away, yet they are solid. So blame the virus we must.
The graphs reveal that
You are only 77% as likely to get COVID if you are not “up to date” with a bivalent booster than if you got a bivalent booster.
No matter whether you get tested a lot or a little, the increased risk in the bivalently boosted holds firm
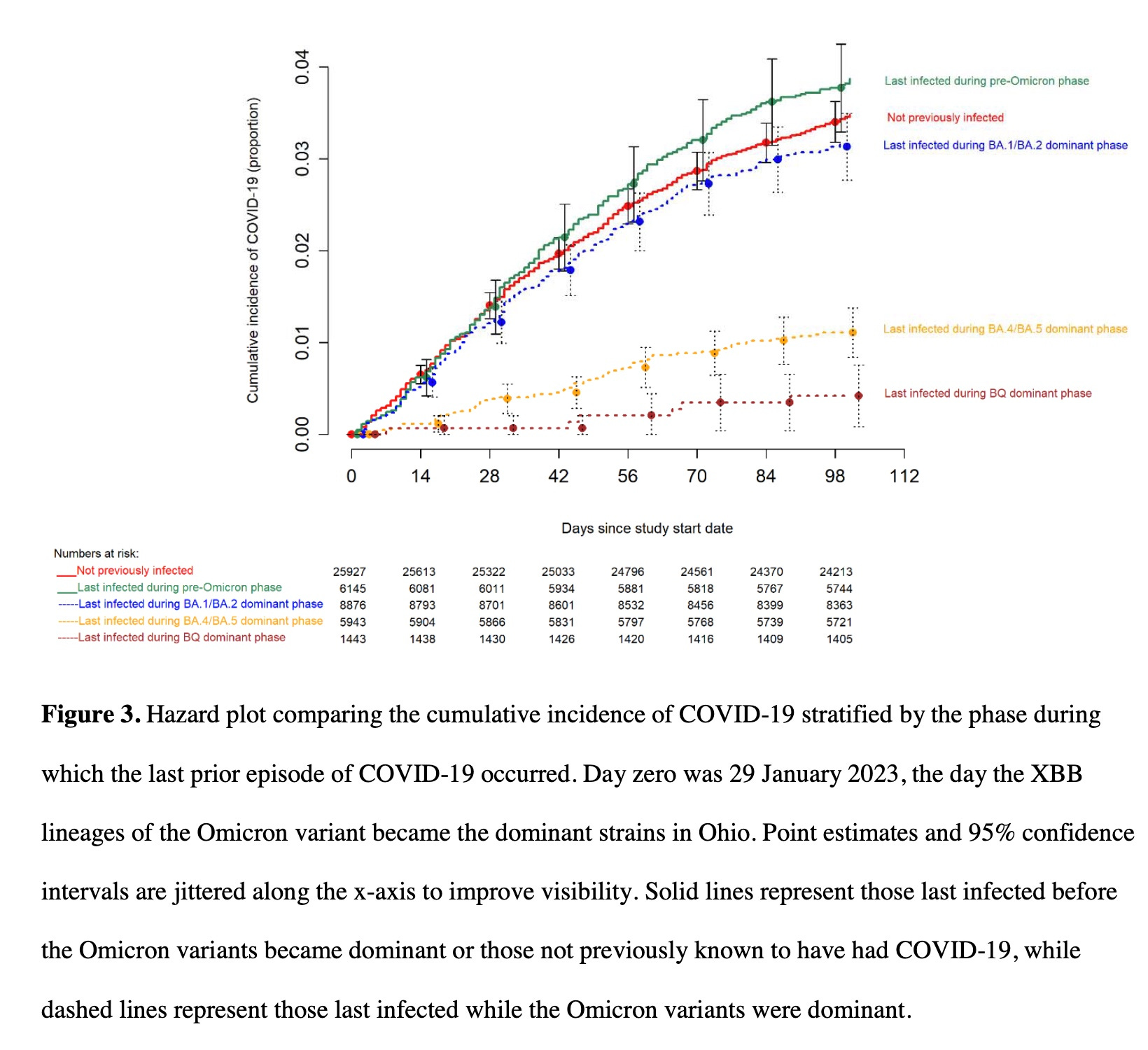
In those previously infected, the longer the period of time since you were infected, the more likely you are to be reinfected—except in those never infected, the risk of infection falls between those who were last infected before omicron and those who were infected with an early omicron variant.
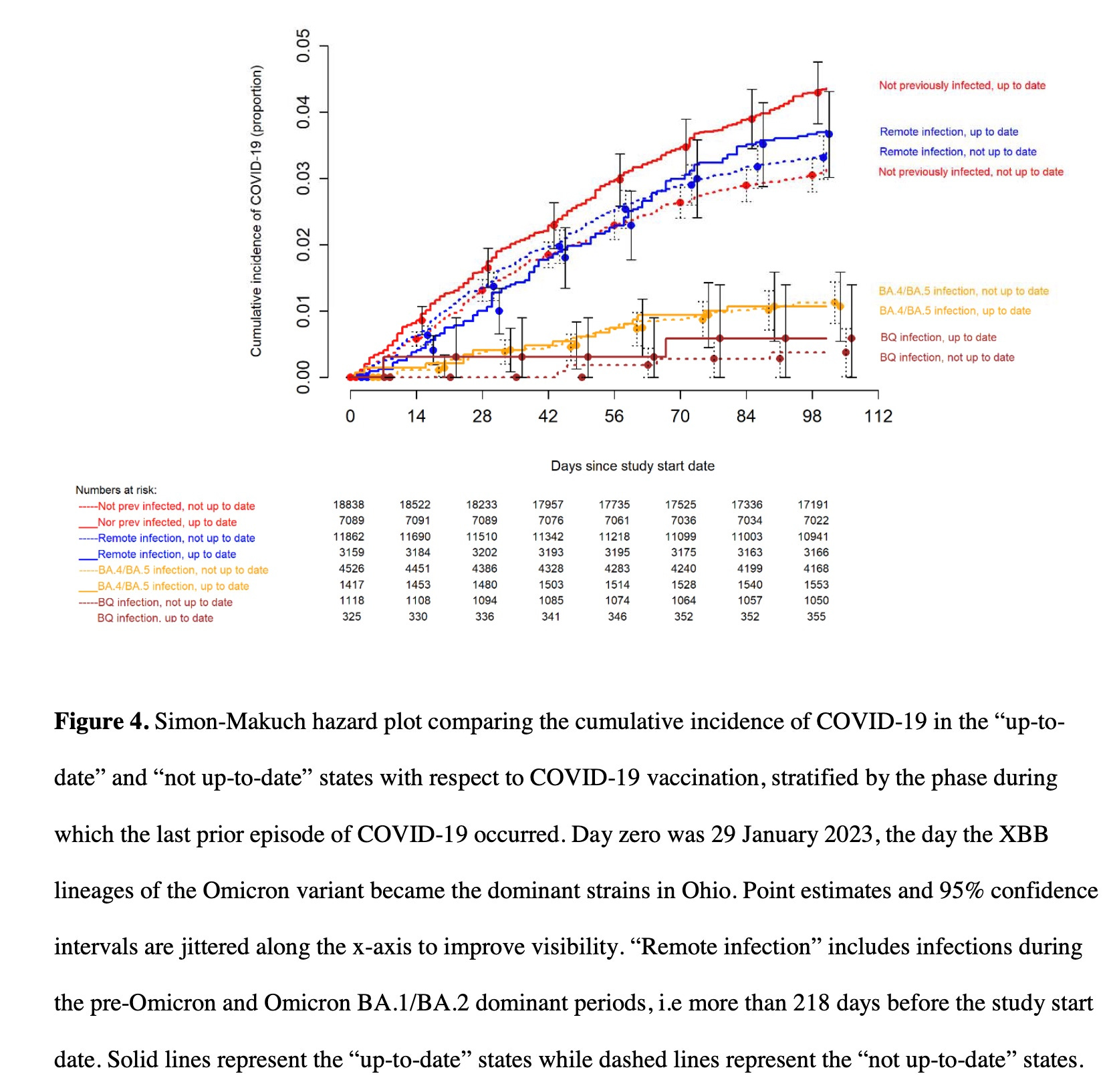
When the distance since the last infection was coupled with whether employees were up to date on a bivalent booster, those who recently had an infection did better and those without a bivalent vaccine did better, consistently.
What this means is that hybrid immunity is yet another phony concept: that it takes an infection plus vaccination to give you stronger immunity is a tall tale.
The 4th graph below reveals that those who were previously infected without receiving a bivalent booster were infected at a lower rate than those previously infected who were also boosted.
“Hybrid immunity” was coined as being something relevant for COVID protection when the bivalent boosters were authorized at the end of August 2022. But it was just another lie. Our federal public health agencies (and those of Canada, the EU, the UK and Switzerland) have morphed into federal public spin agencies—all rolling out bivalent boosters at the same time, all without reliable evidence of anything.
Best to assume the opposite of whatever they claim these days. Please review the long list of lies and obfuscations issued by CDC and FDA which I discussed in early September last year here and then here and here. Please stay away from all their vaccines. They have worked hard and consistently to convince us they deserve our mistrust.
Discussion
In conclusion, this study found that not being “up-to-date” on COVID-19 vaccination by the CDC definition was associated with a lower risk of COVID-19 than being “up-to-date”. This study highlights the challenges of counting on protection from a vaccine when the effectiveness of the vaccine decreases over time as new variants emerge that are antigenically very different from those used to develop the vaccine. It also demonstrates the folly of risk classification based solely on receipt of a vaccine of questionable effectiveness while ignoring protection provided by prior infection.



















No comments:
Post a Comment