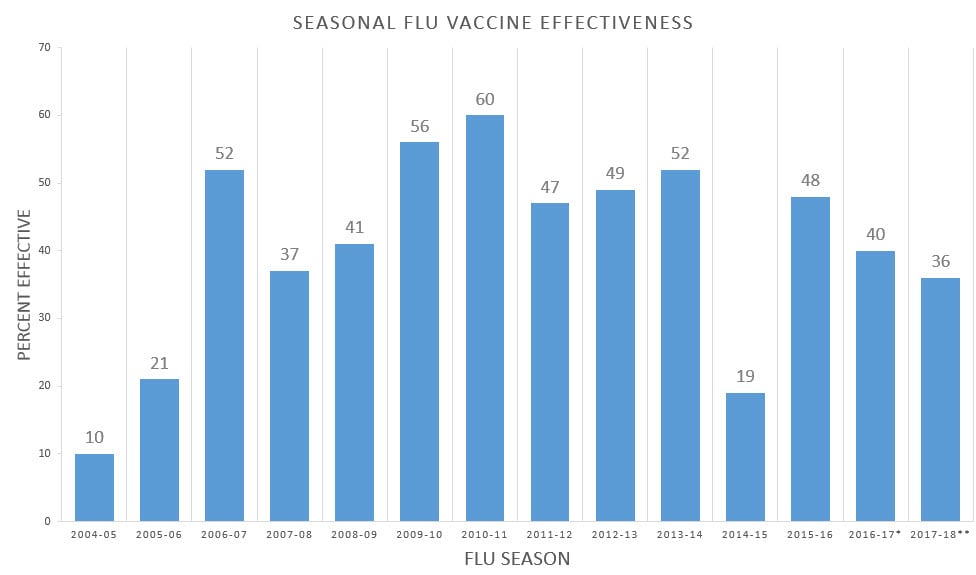
The CDC website posts information for each of the last 14 flu seasons on the effectiveness of each year's flu vaccine. Averaged out, the effectiveness of flu vaccines is 40.5%.
Figure. Effectiveness of Seasonal Flu Vaccines from the 2004-2018 Flu Seasons
While that may not sound too bad, it means that 60% or 3 out of every 5 people who get the shot will not get protection. Yet they are equally at risk of harms from the vaccine as the 2 out of 5 who may benefit.
Only between 3% and 5% of an unvaccinated population will be come down with a case of flu each year, according to the Cochrane Collaboration. Therefore, only 40% of 3%--5% (or a total of 1.2%--2.0%) of a 100% vaccinated population will actually be prevented from getting flu by their vaccination. Stated another way, 98.0-98.8% of those vaccinated get no benefit from their shot each year.
CDC cherry picks the data presented in its chart and graph, choosing only one study per year, or no verifiable study, referring to "unpublished final estimates." How accurate is CDC's claimed effectiveness? Well, the most recent, 2017-18 flu shot is said to have been 36% effective in the US. But in Australia, it was only 10% effective.
In a recent article on flu vaccines in the New England Journal of Medicine, final author Tony Fauci (America's top infectious disease doctor under Obama) cited the 10% effectiveness number to describe last winter's flu shot. He's not buying CDC's fluff.
What about herd immunity from the flu shot? Well, when 6 out of 10 recipients (or maybe 9 out of 10) are not protected, there is no herd immunity. No way to achieve it. Influenza will spread through the population, year after year, no matter how many vaccinations are given.
What about all those nurses and doctors and paraprofessionals who have to get a flu shot or wear a mask continuously during the six months of flu season? Well, 60% of flu shot recipients (or more, depending whether you believe the data from Australia or from the CDC) will get no protection.
As for the professionals wearing masks, which expert among us honestly thinks the mask protects patients, when the masked professional is not sick? None. Obviously, the mask is intended as a badge of shame for the unfortunate employee who dared refuse their vaccination. Will the mask protect patients when the medical professional is sick? The sorry answer is that no one actually knows--but why are they at work if they may transmit a disease?
There are no data that support healthcare professionals wearing masks all winter if they are not vaccinated. Furthermore, CDC notes that only ill healthcare workers should be masked:
If symptoms such as cough and sneezing are still present, HCP [health care personnel] should wear a face mask during patient care activities.In CDC's Interim Guidance for the Use of Masks to Control Seasonal Influenza Virus Transmission, updated in 2018, there is no mention of masking of healthy healthcare workers as a means of flu prevention. Masking of unvaccinated employees is simply a punitive measure imposed by a healthcare establishment that long ago lost its way.
And what about the vaccinated worker who does not wear a mask, but is likelier-than-not to be without vaccine-induced protection? Does she come to work sick, thinking she is protected from flu? Will she avoid wearing a mask when she needs one, so she is not confused with those employees who are being shamed?
Come to find out, years back the vaccine-strain viruses mutated, further reducing effectiveness. And current manufacturing practices are the cause.
"It's been apparent over the last 10 years that egg adaptations have affected the efficacy of flu vaccines," according to Rice University Professor Michael Deem.and
Due to the mutation, most people receiving the egg-grown vaccine did not have immunity against H3N2 viruses that circulated last year, leaving the vaccine with only about 30 percent effectiveness.This problem has been known about since at least 2014, but so far nothing has been done about it. No matter; fuggetaboudit; and in the phrase TV doctor Nancy Snyderman made famous, "Get your damn shot!" In case you haven't noticed, mandating flu shots isn't about science. It's about control.