If I were writing 100 years ago the title of this story would be "Repent"
A worthless piece of pseudo-research on physicians spreading misinformation online was carried out by 2 young women with BS degrees and supervised by an MD, PhD professor at the University of Massachusetts. It wound up in a top journal (JAMA Network) on August 15—but no one seems to know how it could have possibly gotten there. And the ‘study’ claims there was no outside funding. So who paid for it?
I was quoted last week in The Defender about this article.
https://childrenshealthdefense.org/defender/jama-doctors-covid-misinformation/
The JAMA paper has actually garnered quite a bit of press. The methodology seems to be random (“mixed methods study” is what the authors call it). The 2 young first authors trolled social media to collect a list of 52 doctors who provided alternative COVID narratives, and misinformation was DEFINED by any disagreement with the CDC.
I am writing about this because there is an extraordinary, tragic and infuriating backstory to this article that I was not aware of until now.
Design, Setting, and Participants Using US Centers for Disease Control and Prevention guidelines for the prevention and treatment of COVID-19 infection during the study window to define misinformation, structured searches of high-use social media platforms (Twitter, Facebook, Instagram, Parler, and YouTube) and news sources (The New York Times, National Public Radio) were conducted to identify COVID-19 misinformation communicated by US-based physicians between January 2021 and December 2022. Physicians’ state of licensure and medical specialty were identified. The number of followers for each physician on 4 major platforms was extracted to estimate reach and qualitative content analysis of the messages was performed…
Results The propagation of COVID-19 misinformation was attributed to 52 physicians in 28 different specialties across all regions of the country. General misinformation categories included vaccines, medication, masks, and other (ie, conspiracy theories).
Conclusions and Relevance In this mixed-methods study of US physician propagation of COVID-19 misinformation on social media, results suggest widespread, inaccurate, and potentially harmful assertions made by physicians across the country who represented a range of subspecialties. Further research is needed to assess the extent of the potential harms associated with physician propagation of misinformation, the motivations for these behaviors, and potential legal and professional recourse to improve accountability for misinformation propagation.
The only way the medical boards can justify punishing doctors like me, Pierre Kory, Peter McCullough, Paul Marik, Sherri Tenpenny, Paul Thomas etc. etc. etc. is by saying we HARMED someone. This article is attempting to buttress those false assertions and does its best to call for laws against misinformation and more punishments for doctors who stray from the CDC’s fairytales.
MedPropaganda Today wrote a piece supporting the JAMA article, of course. Its editor-in-chief was the chief “expert” witness against me before the Maine medical board.

Read the Robertson quote at the bottom: “The most common theme in the different posts was discouraging people from getting the COVID-19 vaccine.” This ties into my surprise ending. We were trying to save peoples’ lives and health by warning about the COVID vaccines. Yes, we were, and proud of it. Wish we had saved a lot more.
Some media were actually able to distinguish trash when they saw it. Surprisingly, Bloomberg dissed the JAMA paper, acknowledging that the CDC had been wrong about any number of things regarding COVID. It even admitted there could be honest scientific disagreement, something the JAMA paper’s authors never heard of.

Why in heaven’s name, in August of 2023, when most people have learned so much about the lack of benefit of masks, vaccines, lock-downs, “approved” drugs, etc., is this archaic paper coming out now, with its easily disputed claims about what constitutes misinformation?
Corresponding Author: Sarah L. Goff, MD, PhD, Department of Health Promotion and Policy, School of Public Health and Health Sciences, University of Massachusetts, 715 N Pleasant St, Amherst, MA 01002 (sgoff@umass.edu).
Author Contributions: Dr Goff had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Mss Sule and DaCosta are considered co–first authors.
Concept and design: Sule, Gilson, Goff.
Funding/Support: The study was funded via internal support by the University of Massachusetts (Dr Goff).
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer: The views expressed here are those of the authors and do not represent the official policy or position of the US Department of Veteran Affairs or the US government.
Note that the above is contradictory. Professor Goff is responsible for concept and design, also for funding, and yet it says the funder had no role in the design and conduct of the study. And if the study was self-funded by Dr. Goff and U Mass, why add a disclaimer about the US government and the VA? Something is not right.
The conclusions of the JAMA paper are as nasty as expected:
Discussion
This study was the first, to our knowledge, to identify the types of COVID-19 misinformation propagated by US physicians on social media and the platforms they used, as well as characterize the physicians who spread the misinformation. The content of misinformation physicians spread was similar to the misinformation spread by others; this study contributes new information about the range of specialties and regions of the country the physicians represented. The widely varying number of followers on social media for each physician suggested that the impact of any individual physician’s social media postings also may vary.
Some of the physicians identified belonged to organizations that have been propagating medical misinformation for decades,10 but these organizations became more vocal and visible in the context of the pandemic’s public health crisis, political divisiveness, and social isolation. Understanding the motivation for misinformation propagation is beyond the scope of this study, but it has become an increasingly profitable industry within and outside of medicine. For example, America’s Frontline Doctors implemented a telemedicine service that charged $90 per consult, primarily to prescribe hydroxychloroquine and ivermectin for COVID-19 to patients across the country, profiting at least $15 million from the endeavor.29 Twitter’s elimination of safeguards against misinformation30 and the absence of federal laws regulating medical misinformation on social media platforms suggest that misinformation about COVID-19 and other medical misinformation is likely to persist and may increase. Deregulation of COVID-19 misinformation on social media platforms may have far-reaching implications because consumers may struggle to evaluate the accuracy of the assertions made.31
National physicians’ organizations, such as the American Medical Association, have called for disciplinary action for physicians propagating COVID-19 misinformation,32 but stopping physicians from propagating COVID-19 misinformation outside of the patient encounter may be challenging.33 Although professional speech may be regulated by courts34 and the FDA has been called on to address medical misinformation,16 few physicians appear to have faced disciplinary action. Factors such as licensing boards’ lack of resources available to dedicate toward monitoring the internet35 and state government officials’ challenges to medical boards’ authority to discipline physicians propagating misinformation36 may limit action.
Scientific evidence depends on a body of accumulated research to inform practice and guidelines and the evidence depends on the best quality research available at any given time. A recent Cochrane Review has been misinterpreted to have definitively shown that wearing masks does not reduce transmission of respiratory viruses and has been used to support assertions that masks definitively “do not work.”37 Although the Federal Bureau of Investigation and Department of Energy presented a theory to Congress that the COVID-19 virus was the result of a laboratory leak,38 scientific evidence and a more recent report from the Office of the Director of National Intelligence demonstrate lack of evidence for a laboratory leak and favor a zoonotic origin of the virus.39,40 These recent challenges to prior understandings illuminate the importance of transparency and reproducibility of the process by which conclusions are drawn…
Conclusions
Results of this mixed-methods study of the propagation of COVID-19 misinformation by US physicians on social media suggest that physician-propagated misinformation has reached many people during the pandemic and that physicians from a range of specialties and geographic regions have contributed to the “infodemic.” High-quality, ethical health care depends on inviolable trust between health care professionals, their patients, and society. Understanding the degree to which the misinformation about vaccines, medications, masks, and conspiracy theories spread by physicians on social media influences behaviors that put patients at risk for preventable harm, such as illness or death, will help to guide actions to regulate content or discipline physicians who participate in misinformation propagation related to COVID-19 or other conditions. A coordinated response by federal and state governments and the profession that takes free speech carefully into account is needed.
After Pierre Kory told me that he was one of the 52 doctors identified in this ‘study’ I went back and read all the excerpted doctor comments and found that I too was one of the identified 'misinformationists.' I wonder who really paid the cost of the study, which included the creation of the bad doctor list? Professor Goff? UMass? The USG? The VA? I wonder who the list of us got circulated to.
_______________________________
Dr. Goff made a terrible mistake. It was a lot more horrible than producing this silly article. She made an understandable error of judgement two years ago, and it had the most awful result possible. It killed her only child.
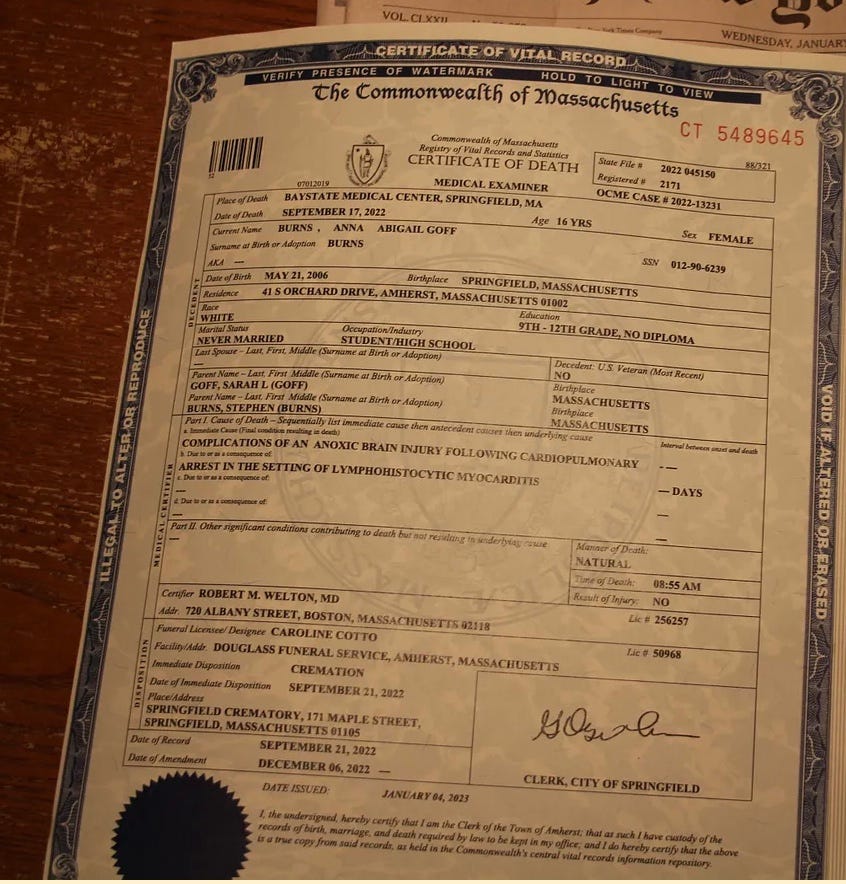
I have written about this story previously, but from a different perspective. Dr. Sarah L. Goff vaccinated her only child for COVID, a beautiful daughter attending Amherst High School, and that child suffered a sudden death at a high school track meet last year.
Not only that, but her daughter had an autopsy, and the cause of death was lymphohistiocytic myocarditis. Certainly the preponderance of evidence—a 99% probability, is that this was a vaccine death due to a COVID vaccine. Everyone must know this, yet Dr. Goff pretends otherwise.
And so instead of warning other parents about the dangers of COVID vaccines, Dr. Goff has funded a “study” to encourage the authorities to hunt down doctors like me for warning other parents not to do what she did.
It must be horrible to know your minor lapse in judgement led to your child’s death. I know Polly Tommey, my colleague at CHD-TV, has a very hard time living with her decision (resulting in an autistic son) and feels called to warn others constantly.
Dr. Goff, however, has chosen the opposite path, to strike out against those of us spreading the warning. Her paper mentions the motivations of us, suggesting it is profit. Really? When it leads to loss of career? How about some honesty, doctor?
She feels free to talk about my motivations (incorrectly) so I feel entitled to talk about hers.
Dr. Sarah L. Goff uses a number of defense mechanisms, which have allowed her to keep her guilt at bay. I think I understand it, but her method of attacking the truth tellers is so harmful, especially when new COVID vaccines are to roll out next month, and could even be mandated for children, that she must be called out. I have much to say to her:
Dr. Goff, stop trying to shoot the messengers who could have saved your daughter, if you had not been deaf to our entreaties. You are using some or all of the following Freudian defense mechanisms to deal with your grief, pain and guilt: denial, repression, projection, displacement, rationalization, sublimation and reaction formation. Get yourself the help you need. You did not mean to hurt her, it was not your fault, it was a tragic accident. You have suffered enough. You can let it go. Get the help you need to do so.
You don’t need to encourage anyone else to be harmed, now that you know the possible consequences. Stop now. I hope God helps you.
[She is not alone. Drs. Peter Hotez and Paul Offit are said to have autistic children, likely as a result of vaccine injuries. They too strike out in exactly the same ways to control their own pain and guilt, as the most aggressive vaccine pushers in the US. Let’s hope they all wake up soon.]