The gray dotted line represents the 5 through 11 age group. It hugs the X axis, and has already dropped back to baseline since its slight uptick in the summer. The aqua line represents the 18-49 year group, the navy line represents the 50-64 year group and the red line 65 years and above.
These graphs and detailed reports from pediatric hospitals, including the report by Lauren Kushner et al., '“For COVID” or “With COVID”: Classification of SARS-CoV-2 Hospitalizations in Children" make clear that hospitalization rates due to COVID are essentially negligible in this age group, even during peaks of infection. The reason CDC could claim steep increases in pediatric hospitalizations was because even a handful of additional hospitalizations caused a marked increase in the rate, and because it included hospitalizations in which COVID was an incidental finding. f. Regarding MIS-C, this is a problem whose dimensions are uncertain, and for which the role of vaccinations is unknown.
2. Pediatric vaccinations cannot be justified as necessary for herd immunity, when herd immunity itself is impossible to achieve with current vaccines. Vaccinating children to protect adults is also unethical.
a. Given the rapid waning of protection and the inability of current vaccines to prevent transmission of SARS-CoV-2, admitted by CDC Director Walensky, it is not possible to achieve herd immunity with vaccination. In fact, the UK's head of the Oxford Vaccine Group, Professor Sir Andrew Pollard, told Parliament that herd immunity due to vaccination was a myth, and "not a possibility." b. While protecting the elderly has sometimes been used as the justification for vaccinating children (for example, against influenza) it is unethical to have one group take on risk to protect another group. It is even more problematic when the group being asked to assume the risk, children, cannot give informed consent. When the magnitude of the risk is significant (of myocarditis, for example) but has not been quantified, and the long-term risks of vaccination are unknown, demanding children shoulder this risk for others is ethically untenable.
3. We know nothing about the long-term risk of vaccination in children. The myocarditis risk immediately after vaccination in older children is considerable, potentially life-threatening, and increased exponentially with decreasing age.
a. The risk might be very high. The pediatric clinical trials are too small to quantify the risk from myocarditis and quantify the risk of most other adverse events.
FDA acknowledged, in its approval letter to BioNTech, c/o Pfizer on August 23, 2021, that it was unable to assess the "known serious risks of myocarditis." "We have determined that an analysis of spontaneous post-marketing adverse events reported under section 505(k)(1) of the FDCA will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.
Therefore, based on appropriate scientific data, we have determined that you are required to conduct the following studies..."
FDA told BioNTech-Pfizer that since FDA was unable to assess the myocarditis risk, it expected BioNTech-Pfizer to do so. FDA wants Pfizer's final reports on myocarditis to be submitted in 2024, 2025 and 2027. Do you think it is okay to vaccinate tens or hundreds of millions of the world's children before BioNTech-Pfizer tells us to what extent their vaccines damage childrens' hearts?
b. According to the Jerusalem Post on October 7, 2021, the health ministry was considering whether "individuals vaccinated with the Pfizer coronavirus vaccine may be asked to avoid strenuous exercise [including swimming] and other physical activity for one week after receiving each dose due to cases of myocarditis..."
c. Let's review some of the data that has been presented at VRBPAC and ACIP meetings this year.
Confining ourselves to males who received a 2nd dose of an mRNA vaccine and reported myocarditis within a week of the shot to VAERS, we see that the reported myocarditis rate in the age group 12-17 (62.7/million) was over 100 times greater than in the over-65 group (0.6/million). Graphing these rates (below) we see that the rates increased exponentially as age decreased. Extrapolating from this graph we could expect the highest myocarditis rates in younger children.
Tweeting
from the October 21, 2021 ACIP meeting, esteemed reporter for Stat, Helen Branswell, informed us that the rate of myocarditis in military servicemembers under age 20 was over 100 cases per million. The third graphic is the report to VAERS of a death in a 15 year old, attributed to myocarditis, six days after receiving a COVID vaccination.
FDA's Doran Fink pointed out at a recent meeting that we have no idea of the rate of subclinical myocarditis. Nor are there good data regarding the long-term sequelae of COVID vaccine-induced myocarditis in teens or other children. Recall that a 2015 military study by Renata Engler et al. revealed a rate of subclinical myocarditis after a 1st smallpox vaccine to be one in thirty. 4. The evidence suggests that Pfizer is neither reliable nor trustworthy
a. Pfizer is projected to earn $33 billion dollars this year in vaccine sales, and more than that next year. Do you honestly think Pfizer-BioNTech will try to identify the actual rate of myocarditis in children, when so much money is at stake? I am sure you are aware that Pfizer is the world's largest drug company, and also that Pfizer has paid more in fines to federal and state governments than any other pharmaceutical company.
b. An October 19, 2021 Public Citizen report titled Pfizer's Power, discussing Pfizer and its COVID vaccine contracts notes: "neither Pfizer nor the U.S. government can make “any public announcement concerning the existence, subject matter or terms of this Agreement, the transactions contemplated by it, or the relationship between the Pfizer and the Government hereunder, without the prior written consent of the other.”[28] The contract contains some exceptions for disclosures required by law." I recommend you read the entire brief report to understand the nature of the vaccine company whose product you are dealing with.
5. What we don't know yet, or haven't been told, is critically important. Why rush the shots into children?
a. Four Nordic countries recently halted the use of Moderna's vaccine in some age groups due to the risk of myocarditis. It was reported by the Wall Street Journal that FDA paused its review of the Moderna vaccine for teenagers in response to the Nordic countries' action. The article was subtitled, "Agency holds off decision on expanding use of shots to 12-to-17-year-olds while it looks into risk of rare heart condition."
Shouldn't FDA hold off its expansion of the Pfizer shot to 5-11 year olds, since Pfizer's shot also causes myocarditis, until it has completed this review?
b. The VAERS data on myocarditis are clearly concerning. The absence of data from other FDA and CDC- accessible databases ought to be alarming. When 60% of the US has been vaccinated, how can it be that we still do not know the actual rates of myocarditis in the population? Is this information being concealed in order to garner authorizations for the vaccines in the pediatric population?
c. Other information from VAERS ought to have raised an alarm long ago. How can it be that adverse event reports input to VAERS are greater, since the COVID vaccines were rolled out, than all cumulative AE reports to VAERS for the prior thirty years? Death reports for 2021 are also greater than cumulative deaths reported to VAERS over the preceding 30 years.
Why has no public health official explained this? Why has CDC, which is charged with investigating every reported death in VAERS, simply waved its hands and claimed none are due to vaccination, without providing any data? d. The bottom line is that we have no idea of either the short or long-term risk of the Pfizer vaccine in 5-11 year old children, but it is reasonable to assume the risk of myocarditis could be considerable. Other risks have not been quantified but could also be considerable. Yet we do not even know their magnitude in adults, after 6.8 billion COVID vaccinations have been administered throughout the world. How can anyone possibly justify vaccinating children with vaccines for which the world's public health professionals have failed to collect and analyze the most rudimentary data on safety during the largest rollout of (mostly experimental) vaccines in the history of the world? Obviously, policies were put in place such that we will never know the risks of COVID vaccinations nor the magnitude of those risks. Why?
6. The benefit exceeds the risk?
a. In the past, your briefers have exaggerated the harms to children from COVID and magnified the benefits of vaccination in order to claim that benefit exceeds risk. This was accomplished through the use of datasets that inexplicably failed to yield adverse event signals, conflating deaths and hospitalizations "with" COVID as if all were "due to" COVID, ignoring the existence of naturally acquired immunity and making overly optimistic assumptions about the efficacy and duration of vaccine-induced protection. However, if you use more realistic data, such as presented here, the risk exceeds benefit in the 12-15 age group, and will exceed benefit in the 5-11 year age group also.
b. One of your briefers who failed to find adverse event signals in the VSD was Nicola Klein, who is the Principal Investigator (PI) in multiple COVID vaccine studies for Pfizer conducted in both adults and children. Those trials have brought in many millions of dollars to her institution. This conflict of interest was undisclosed.
c. What percentage of young children are already immune? At a June VRBPAC meeting we learned that 27% of children were naturally immune, a higher proportion than in any other age group. They were tested using anti-nucleocapsid antibodies. Since then, they have had a summer in which to play together and two months of in-person schooling, and their immunity could be approaching 50%. Vaccinating these children will expose them to risk without the prospect of benefit. Why do it?
d. FDA allows Pfizer to use anti-nucleocapsid antibody tests to identify prospective subjects for clinical trials who have preexisting immunity; they are not included in the efficacy analysis. Yet FDA and CDC do not allow ordinary American children or adults to use the identical test to demonstrate that they are already immune and don't need vaccinations for COVID. Why do you think this is? Does it make medical or scientific sense? Common sense? Why are Americans forbidden from demonstrating they are immune and can safely go with their life unvaccinated?
e. Didn't you find it surprising that so many federal public health officials claimed that recovered immunity was expected to be weaker than vaccine-induced immunity? Didn't that go against what you learned in medical school? Can everyone finally agree that recovered immunity is broader and longer-lasting than immunity derived from current COVID vaccines? 7. Beware the data tricks being employed to minimize safety concerns
a. You know that VAERS is a passive reporting system that is intended to provide signals of potential safety problems, which must be evaluated with additional studies. You know that VAERS data cannot be used to calculate the rates of any adverse reaction. Yet CDC did exactly that for anaphylaxis, claiming the rate of VAERS reporting was the rate of occurrence. b. When a high quality study of MGH and Brigham hospital employees showed that anaphylaxis occurred in 250 per million employees, CDC failed to update its website and still claims, as of October 18, 2021 that anaphylaxis occurs only 2-5 times per million COVID vaccinees. Which begs the question: how accurate are CDC's other adverse event rates? c. CDC has made a number of changes to its standard practices since the beginning of the pandemic. Here is just one example. Beginning on May 1, 2021, for CDC to accept a report of a breakthrough case, the infected case must have required hospitalization or died and had their infection confirmed with a PCR test using 28 or fewer cycles. Other problems with data acquisition of breakthrough cases have further contributed to keeping the official number of such cases much lower than they really are. In the UK, in all age cohorts of 30 years and up, there is a higher rate of COVID cases in the vaccinated compared to the unvaccinated. d. Maddie de Garay was a healthy 12 year old when she entered Pfizer's pediatric COVID vaccine trial at the University of Cincinnati with her two siblings. She became ill immediately after the second dose with high fever and then a wide range of symptoms. Over the subsequent six months she had about a dozen ER visits and six hospitalizations. She has required a feeding tube to be nourished and uses a wheelchair. Dr. Frenck, the PI, was her physician and is aware of these problems. Yet she was not reported as a serious adverse event in the trial documents, and when her trial was published in the NEJM, there were no serious vaccine-related adverse events listed for any subject. Her physician, Dr. Frenck, was the first author of the NEJM study. How many other subjects in Pfizer's trials were similarly injured, but went unreported? How many Principal Investigators issued positive reports despite knowing of injuries? 8. How many vaccines will children need? What are the cumulative risks? How can we be sure there will be no ADE?
a. None of this is known. Under what conditions is it acceptable to experiment on millions of our children simultaneously?
b. In Israel, the green pass expired after 6 months, and college students have already received a booster dose. As you know, data regarding booster dose efficacy and safety is scanty. Evidence of cumulative dose safety does not exist.
9. Conflicts of interest.
a. We at Children's Health Defense have not devoted ourselves to investigating potential VRBPAC member conflicts of interest (COIs), but we noted that half the voting VRBPAC members are temporary members, presumably installed to replace permanent members who disclosed COIs. Yet 3 current voting members have glaring COIs. Eric Rubin, editor in chief of the New England Journal of Medicine, has published all the Pfizer clinical trials, and the NEJM will have earned a considerable sum for reprints and advertising from Pfizer. Drs. Amanda Cohn and Melinda Wharton are both career CDC employees. Were either of them to vote against a vaccine authorization or approval it could have severe consequences for their careers.
Both Eric Rubin and Melinda Wharton are temporary members. We are dismayed that conflicted temporary members were selected to replaced conflicted permanent members on the VRBPAC.
10. Early treatment works, but to acknowledge this would prevent EUAs from being issued for COVID vaccines and on-patent drugs like Regeneron's monoclonal antibodies, remdesivir and molnupiravir.
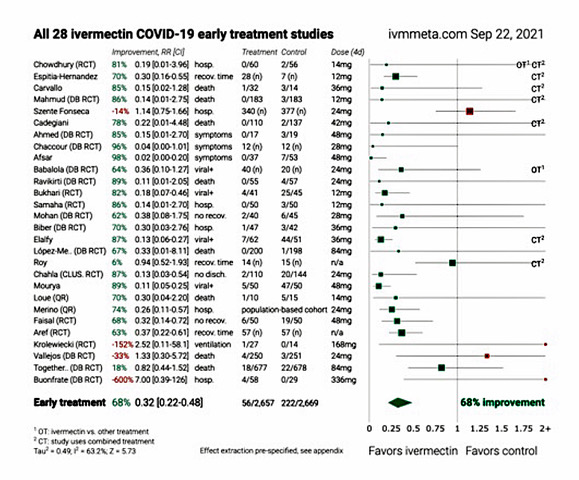
a. The statute under which Emergency Use Authorizations (EUA) are defined requires that there exist no alternative approved, adequate and available product in order for an EUA to be issued. Had effective drugs not been deliberately suppressed, no EUAs could have been issued. b. If children and adults were treated early with proven drug combinations, very few would progress to the inflammatory and thrombotic stage of COVID-19. While this statement may appear controversial, forest plots of the compiled literature on hydroxychloroquine and ivermectin for COVID are very compelling, with average efficacy against the different endpoints of 64% to over 80%. c. The Nebraska Attorney General on October 15 issued an extraordinary 48 page opinion regarding these two drugs, giving safe harbor to medical practitioners and pharmacists who prescribe and dispense them with informed consent. We expect to see more opinions like it as the states protect the public from the harmful acts of health professionals. d. The probable efficacy of chloroquine drugs for coronaviruses was demonstrated in experiments published by the CDC in 2005 and by Dr. Fauci's NIAID in 2014. This prior knowledge, obtained by CDC and NIH regarding these drugs' efficacy at standard doses and their safety at standard doses, while agency officials suppressed their use during the pandemic, is clear evidence of willful misconduct and nullifies liability protection for these federal officials.
11. Spike protein, the putative antigen induced by all 3 COVID vaccines, is a toxin.
It is produced and enters the circulation, has predictable negative consequences to vascular endothelium, activates platelets, and crosses the blood brain barrier. It would be expected to trigger the destruction of cells that produce it and present it on their surfaces. Products that induce the production of spike protein should only be used after careful consideration of the individual recipient's risks and benefits. They should not be employed in mass vaccination programs where there is no learned practitioner to weigh appropriate use, nor in individuals with a very low risk of serious COVID disease.
 b. In the October 2021 Pediatrics a report by David McCormick et al. showed that of 112 pediatric deaths associated with SARS-CoV-2, 86% had comorbidities, especially obesity, neurologic and developmental conditions. The mean age of decedents was 17.[2]
b. In the October 2021 Pediatrics a report by David McCormick et al. showed that of 112 pediatric deaths associated with SARS-CoV-2, 86% had comorbidities, especially obesity, neurologic and developmental conditions. The mean age of decedents was 17.[2]









ReplyDelete'US Sen. Johnson Continues to Press the FDA, Pfizer, BioNTech on Transparency and Politicization of Vaccine Approval Process:'
The senator wrote to Pfizer and BioNTech, “When the FDA made its August announcement it stated although COMIRNATY (COVID-19 Vaccine, mRNA) is approved to prevent COVID-19 in individuals 16 years of age and older, there is not sufficient approved vaccine available for distribution to this population in its entirety at the time of reissuance of this EUA.’ On September 13, 2021, the National Library of Medicine within the National Institutes of Health, reported, ‘[a]t present, Pfizer does not plan to produce any product with these new [Comirnaty National Drug Codes] and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution.’ On September 22, 2021, the FDA reissued the EUA for the Pfizer-BioNTech COVID-19 vaccine, with the same language regarding availability limitations for individuals 16 years of age and older. 'Based on these statements it appears that individuals who are required to be vaccinated under President Biden’s and the Department of Defense’s vaccine mandates' may not be able to receive the fully licensed and "approved vaccine.”
https://www.ronjohnson.senate.gov/2021/10/sen-johnson-continues-to-press-the-fda-pfizer-biontech-on-transparency-and-politicization-of-vaccine-approval-process