The CDC’s Dr. Shimabukuro gave a talk on June 10, 2021 to FDA’s vaccine advisory committee (VRBPAC) discussing preliminary safety data from V-safe, VAERS and VSD. So preliminary it did not agree with what we have learned later. Let’s look at what he said, knowing that by June 10 the regulatory agencies knew a lot more than they were disclosing.
https://www.fda.gov/media/150054/download
Let’s start with his chart on myocarditis cases by age, observed vs expected, after Dose 2. The data were collected through May 31, 2021. There were only 2 cases in 12-15 year olds because there was not enough time for that age group to get their second shot: it was authorized for them on May 10, and they had to wait 3 weeks for the second dose. Three weeks later was May 31, the data cut-off. So there should have been NO myocarditis reports from the 12-15 year age group, because not enough time had elapsed for them to legally receive a second dose. Yet his chart claims 134,000 2nd doses had been administered by May 31. Hmmm.
Also remember that there has been a considerable delay between when patients or HCWs provide a report to VAERS, and when it is electronically entered into the system.
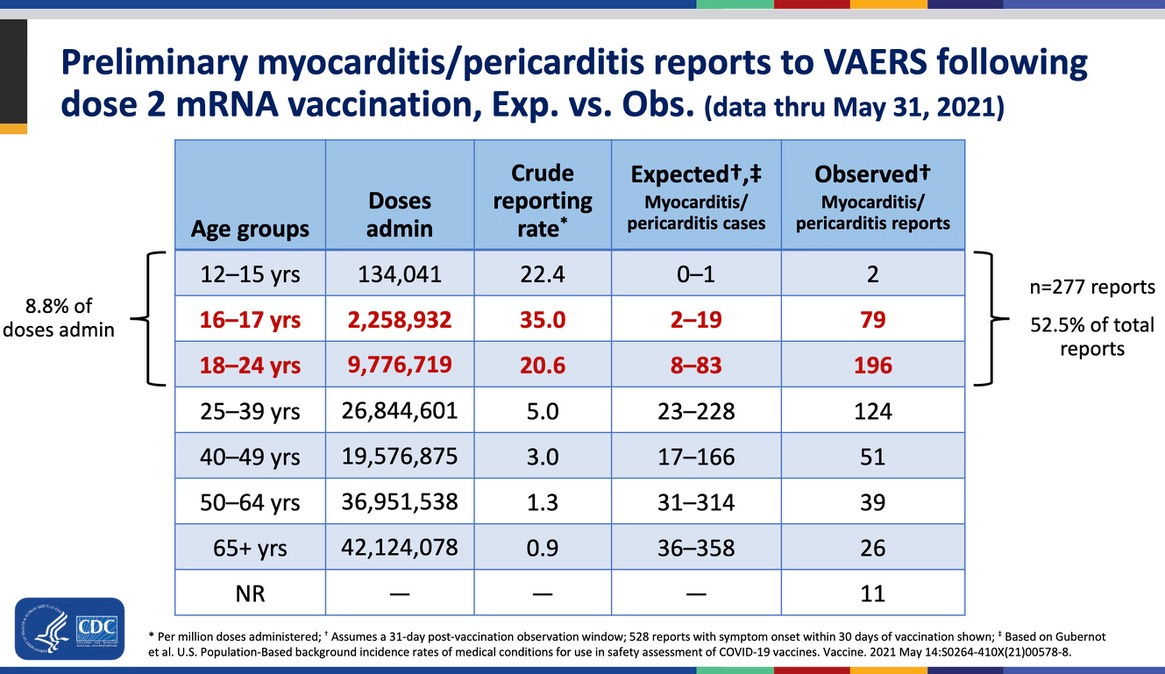
In any event, people under age 25 comprised only 8.8% of the second doses received, but were 52.5% of the myocarditis cases reported. On this basis they were about 6 times as likely to report myocarditis as the whole group.
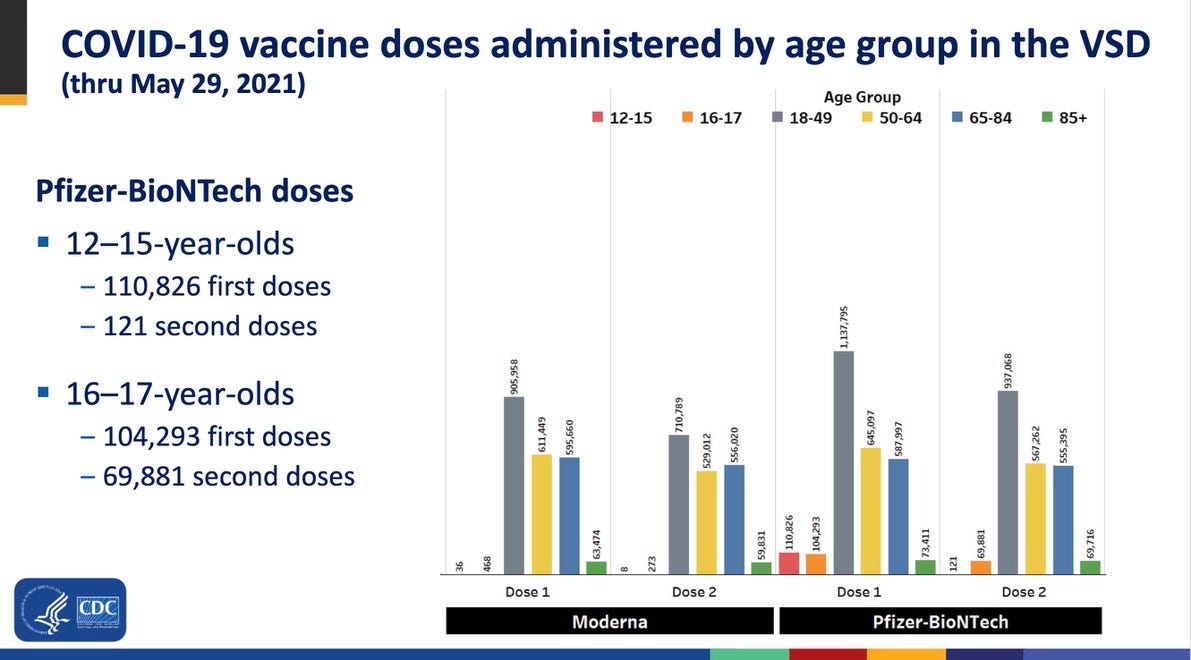
The VSD (Vaccine Safety Datalink) is a collection of HMOs with 12 million members. CDC pays to access their health records. Of those 12 million enrollees, fully 1/3 of the vaccinated 16-17 year olds did not go back for their second dose. Presumably most had a troublesome adverse reaction.
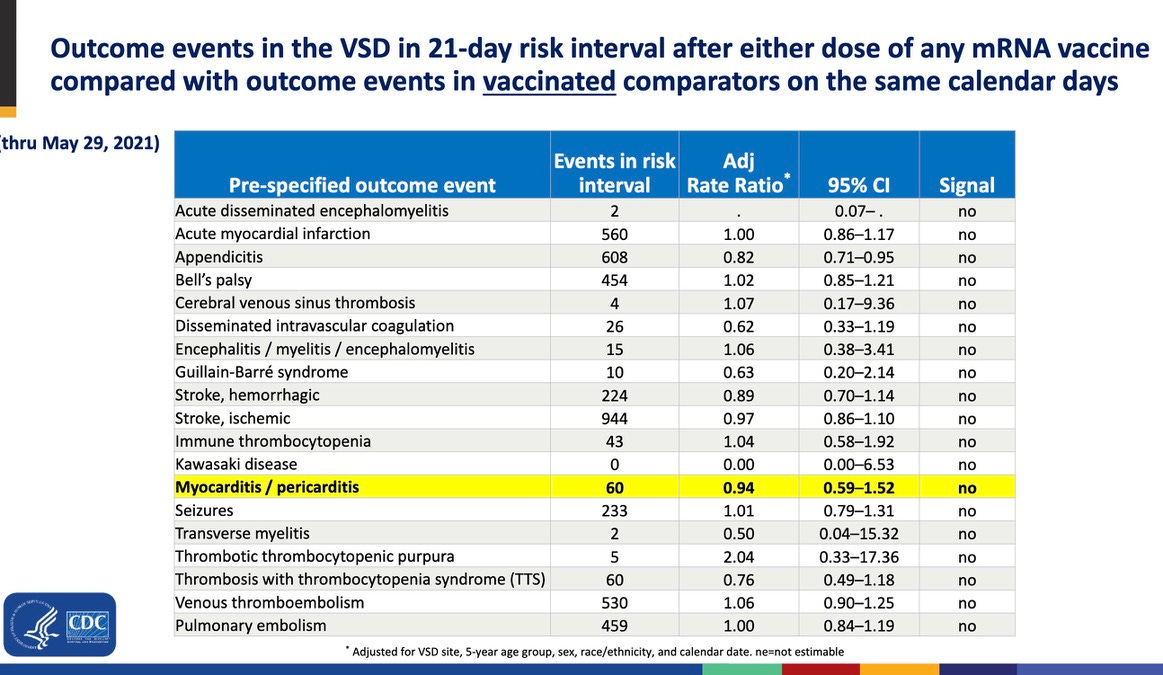
The below slide is etched in my mind from that meeting. I do not believe it could be accurate. Either the numbers, or the way they were analyzed, is wrong. Dead wrong. This slide claims that people given other vaccines were more likely to get myocarditis than those who got a COVID vaccine. Hello? Not possible. The only other vaccines that commonly cause myocarditis are smallpox ad monkeypox, and neither was being given to civilians at that time.
It claims that all the ‘adverse events of special interest’ which are called the more benign-sounding ‘prespecified outcome events’ below, are unassociated statistically with COVID vaccines, based on what ought to be a robust (and highly vaccinated) 12 million person dataset. Not even one of the adverse events the CDC thought were most likely associated with COVID vaccines had generated a safety signal by May 29, 2021 in the VSD. Or so the CDC claimed.
In the next slide Dr. Shimabukuro says there were only 22 cases of diagnosed myocarditis in 16-39 year old enrollees in the VSD. 18 occurred after the second dose. 14 were in those who received Moderna.
But here is something strange. Even though 11 episodes of myocarditis occurred after the second Moderna dose, there is a claim that the adjusted rate ratio (ARR) is “non-estimable.” Yet Dr. Shimabukuro estimated the ARR for Pfizer’s first dose when there was only 1 myocarditis case. Furthermore, the confidence interval looks sound, starting above 1. I think they did not want us to see the ARR for myocarditis associated with Moderna’s second dose, because it would have been sky-high. (Note that in studies from many countries, the Moderna vaccine is much more strongly associated with myocarditis than the Pfizer vaccine. Note also that the DHHS is a patent holder for Moderna’s vax but I do not think it is for Pfizer’s.)

Below it is clear that even by May 29 the second dose caused over 5 times as many myocarditis cases as the first dose. For both brands. And these data have been repeated all over. This cannot be a random event.

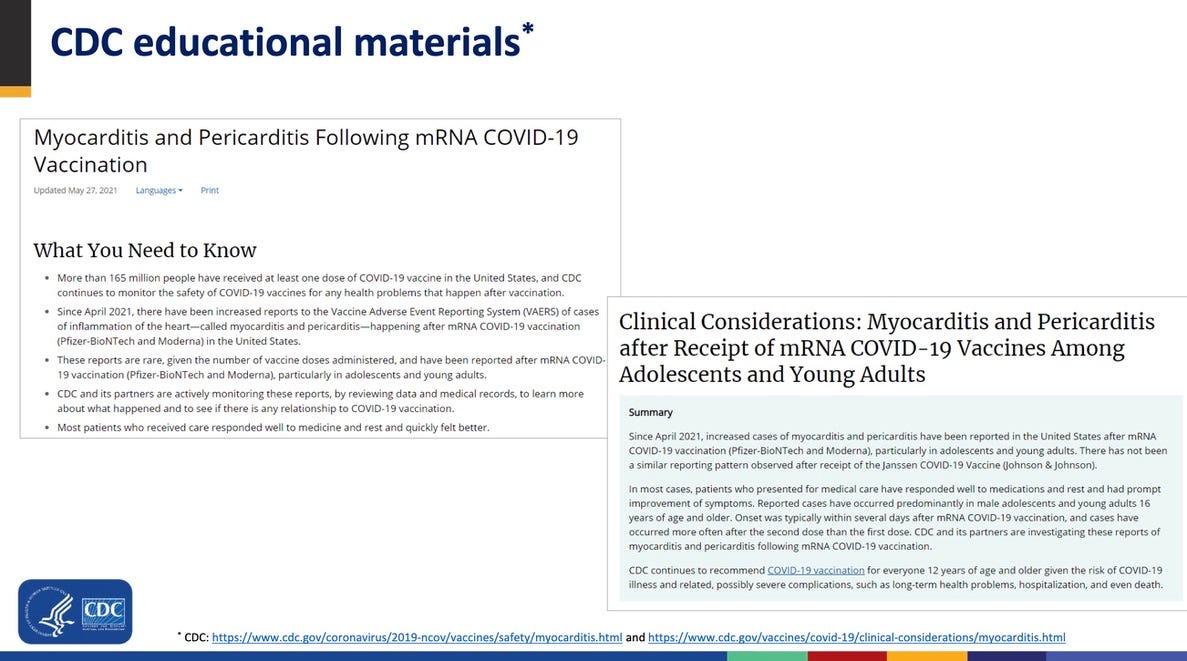
Below, I show you how hard the CDC worked to cover its derriere regarding the myocarditis “signal” — I would call it a criminal coverup — regarding the data it was sitting on, and other data it was misrepresenting. On May 27, 2021 CDC updated its guidance regarding myocarditis and pericarditis, according to the slide below. The slide gives you 2 URLS where you can find the educational materials CDC created.
However, neither of those URLs is operative any more. And when I tried to find them on the WayBackMachine, somehow they just were not archived…. So, where is the evidence that CDC warned anyone on May 27 about the risk of myocarditis? Why has it disappeared off the internet?
Did CDC send out an emergency warning to their network, the way they did when two people who obtained ivermectin from a feed store and on the internet required hospitalization for apparent overdoses? No.
The Fact Sheets that substitute for an informed consent, and are required to be given to all vaccine recipients, should have been updated with this warning immediately, according to the Prep Act. It requires that significant known risks be disclosed. I’d call heart damage and the risk of sudden death significant.
Summary: Dr. Shimabukuro did the CDC tap dance in his summary, which goes like this: “Initial safety findings… are consistent with results from pre-authorization clinical trials.” What does that mean? It means, ‘We already knew about this, we are not concerned, nor should you be.’ Tap dance two: this is just preliminary, we are continuing to scour the data, and we will tell you more in 8 days at the scheduled ACIP meeting. (I think it was postponed, however, while the spin doctors worked overtime crafting a new narrative.) The bottom line was ‘nothing to see here.’
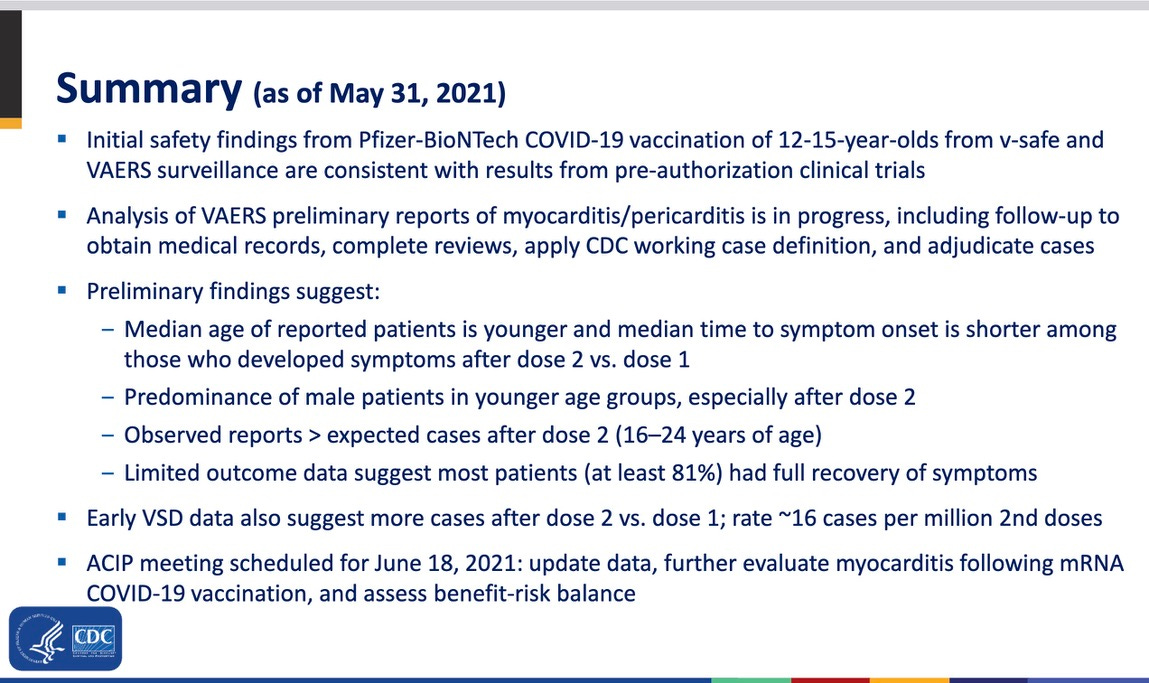
And just in case you were not convinced, this is the most intensive vaccine safety monitoring in US history.
And I LOVE the acknowledgements. CDC pretty much always acknowledges the people who contributed to a presentation or to a research project. But here, the people are missing. Only the agency and subagency names are given.
Do you think an executive decision was made to shield the bureaucrats who created this misleading presentation? I wonder if Dr. Shimabukuro has received any monetary awards from CDC recently.
Early in this talk, Dr. Shimabukuro showed the following slide. Think about it. After his presentation went through multiple layers of review, the CDC tools still felt the need to shift any and all blame to poor old Dr. Tom Shimabukuro. Nope. Not their agencies. They didn’t hide anything….
ReplyDelete"203 ivermectin COVID-19 studies, 155 peer reviewed, 96 comparing treatment and control groups.
Ivermectin was adopted in all or part of 22 countries (39 including non-government medical organizations). Submit updates/corrections.
https://c19ivm.org/