Let's start with tetanus, the disease we think of when scratched with something rusty or dirty, and develop an abscess. This is a terrible illness, because tetanus bacteria produce a nerve toxin that takes months to recover from.
First, how much tetanus disease is there is the US? Second, does it spread from person-to-person? There are about 30 cases and 4 deaths per year in the US. Most cases occur in those over 35 years old. Tetanus comes from a wound. it does not spread from one person to another.
Tetanus - United States, 1947-2008
FIGURE. Annual rate* of tetanus cases and tetanus deaths --- National Notifiable Diseases Surveillance System, United States, 1947--2008
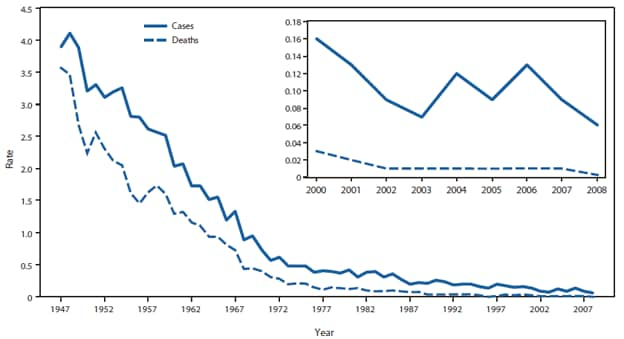
* Per 1 million population.
Alternate Text: The figure above shows the annual rate of tetanus cases and tetanus deaths in the United States during 1947-2008, according to the National Notifiable Diseases Surveillance System. From 1947 to 2008, the number of tetanus cases reported each year, which already had decreased greatly since 1900, continued to decline
Diphtheria - United States, 1980-2011
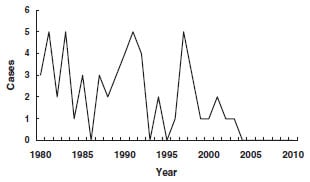
What about diphtheria? Since 1980, there have been 5 or less US cases yearly per CDC's chart, here. You child will virtually never be exposed. But here is a surprise from the medical textbook "UpToDate". The vaccine is not that effective, since it immunizes against a toxin but not against growth of the bacteria that produce the toxin:
So we are currently protected by the low level of toxin-producing diphtheria strains in the environment, and only to a small degree by the vaccine itself. By serology, 91% of children aged 6-11 had protective diphtheria antibodies, but only 30% of adults over 70 had protective antibodies. If we were worried about plugging immune "holes" we would start vaccinating adults, not children. But we don't need to, because the environment protects us from diphtheria, with help from the vaccine, in today's era. See this abstract from the US Center for Health Statistics, 2002:"Asymptomatic carriers are important for transmission of diphtheria. Immunity (either via natural infection or vaccine-induced) does not prevent carriage. In areas of endemicity, up to 5 percent of healthy individuals may have positive pharyngeal cultures... As the general population becomes immune, there are fewer cases of clinical diphtheria (from toxigenic strains) and less asymptomatic colonization with toxigenic strains and therefore decreased transmission to nonimmune people. However, there does not appear to be any reduction in the prevalence of carriers of non-toxigenic C. diphtheriae. Immunized individuals can develop clinical diphtheria, although disease is less severe and occurs less frequently."
Ann Intern Med. 2002 May 7;136(9):660-6.
Serologic Immunity to Tetanus and Diphtheria in the US
McQuillan GM1, Kruszon-Moran D, Deforest A, Chu SY, Wharton M
Serologic Immunity to Tetanus and Diphtheria in the US
McQuillan GM1, Kruszon-Moran D, Deforest A, Chu SY, Wharton M
- 1Division of Health Examination Statistics, National Center for Health Statistics, Hyattsville, MD 20782, USA. gmm2@cdc.gov
Abstract
BACKGROUND:
OBJECTIVE:
DESIGN:
SETTING:
PARTICIPANTS:
MEASUREMENTS:
RESULTS:
CONCLUSIONS:
Pertussis has re-emerged in the US due to several vaccine failures, particularly because the vaccinated can spread it, while experiencing only minor illness.
The first failure was the low efficacy of the former DPT ("whole cell pertussis") vaccine. Even though CDC admits the DTP vaccine was only 70-90% effective after 4 doses for pertussis, diagnosed pertussis cases dropped dramatically in the US during its period of use. But then they resurged, beginning in the 1970s, despite widespread vaccine use. [Most cases were not diagnosed and reported, since diagnosis required special culture media, and if there had been antibiotic treatment, cultures were generally negative. I and other clinicians have treated a lot of presumed pertussis cases over the last 30 years. There are no reliable case counts. But the trends are accurate, in my view.]
Pertussis - United States, 1950-2010

The second failure was the pertussis vaccine's toxicity: it caused a high rate of seizures and other neurological reactions in children. Once this was acknowledged, a less toxic acellular pertussis component was used in US vaccines, beginning in 1992.
CDC expected the new vaccine to be both safer and more effective than the older vaccine. CDC notes:
"When studied, the [new] acellular pertussis vaccine was significantlymore effective than whole-cell DTP in preventing serious pertussis disease. Protection decreased with time, resulting in little or no protection 5 to 10 years following the last dose."
Drugs and vaccines always look more effective in pre-
licensure trials (sponsored by their manufacturers) than they appear later. Although less toxic, the newer vaccine turned out to be less, not more, effective. Not only did protection wane fairly rapidly; the newer vaccine (compared to the former vaccine) enhanced spread of Bordetella pertussis, according to FDA. From UpToDate:
"...several reports suggest that the immunity following administration of the fifth DTaP dose wanes more rapidly than expected, leaving a gap in immunity between the last childhood dose of DTaP and the Tdap (6th dose) booster vaccine (suggested age of administration at 11 to 12 years of age). Adolescents who received the childhood DTaP vaccine appear to have a substantially higher risk of contracting pertussis than those who received the DTwP [older] vaccine."Despite recommending 2 extra DPT doses (for adolescents and adults) for the vaccine schedule in 2005, CDC recommended that all close contacts of a case of pertussis take prophylactic antibiotics. Close contact includes being in the same room as someone with pertussis for a prolonged period, such as in your child's schoolroom. It seems even with six doses by age twelve the pertussis vaccine is unreliable.
Here's the bottom line: the tetanus component of current DTP vaccines seems to work reasonably well, while both diphtheria and pertussis components offer less protection than desired. They reduce severity but do not prevent infections well; they allow the vaccinated to spread disease, and the protection (certainly for pertussis, and serologically for diphtheria) wears off over several years. A safer and more effective vaccine for pertussis, and a more effective diphtheria vaccine, are needed.
No comments:
Post a Comment