My
comments on the letter are in italics. A preponderance of signers are
from former Soviet countries. Kerry Kennedy, on a mission to embarrass
her older brother, is an outlier.
https://gordonandsarahbrown.com/2024/03/pandemic-accord-joint-letter/
20 March, 2024 5 MIN READ
To Leaders of WHO Member States,
The overwhelming lesson we learned from COVID-19 is that no one is safe anywhere until everyone is safe —no,
the lesson we learned is that all media and public health officials
were handed the identical script and it was all a lie. It was designed
to make us feel guilty about not taking a deadly so-called vaccine.
everywhere – and that can only happen through collaboration. — The
WHO is not asking for collaboration. It is asking to be the arbiter of
supplies, deciding who gets what. The world must obey its commands.
That is not collaboration.
In response, the 194
countries which are members of the World Health Organization decided in
December 2021 to launch negotiations for a new international instrument
on pandemic prevention, preparedness and response, a Pandemic Accord, as
a “global framework” to work together to prepare for and stem any new
pandemic threat, including by achieving equitable access to vaccines, therapeutics and diagnostics.—because
what the globalists want is for no one else, anywhere, to be left behind when the
toxic, liability-free “vaccines” are rolled out next time.
Negotiation of an effective pandemic accord is a much needed opportunity to safeguard the world we live in. Countries
themselves have proposed this instrument, individual countries are
negotiating it, and only countries will ultimately be responsible for
its requirements and its success or failure.—Then why do
the WHO’s funders like Bill Gates’ BMGF and GAVI have a seat at the
negotiating table? Why are hand-picked committees doing the
negotiating? Why is the WHO bureaucracy writing much of the documents?
Why is it Tedros who will issue the orders? Why are we always lied to
about this?
Establishing a strong global pact on
pandemics will protect future generations from a repeat of the millions
of deaths and the social and economic devastation which resulted from a
lack of collaboration during the COVID-19 pandemic. — Actually,
the response (lockdowns, closing businesses and sending people home
without jobs, forcing ventilators and bad drugs and vaccines on the
world) killed many more than the disease did, and it was the WHO
decisions that determined this response.
All
countries need what the accord can offer: the capacity to detect and
share pathogens presenting a risk, and timely access to tests,
treatments and vaccines.—timely access to tests, treatments
and vaccines that were accurate and effective was blocked by the WHO
which supported unreliable tests, bad treatments, and awful vaccines.
If the WHO gains the power to impose its will on the world and there is
no competition within the marketplace, nor liability for the products, we can expect the
tests and treatments to be of even worse quality next time.
An
agreement is meant to be reached just two and a half months from now –
countries imposed a deadline of May 2024, in time for the 77th World
Health Assembly.
As countries now enter what should be the
final stages of the negotiations, they must ensure that they are
agreeing on actions which will do the job required: to prevent and
mitigate pandemic threats. —No one has
produced a shred of evidence that anything suggested in the treaty or
amendments has any chance of preventing a pandemic. Do tell us how that
is supposed to happen, when the WHO is proliferating potential pandemic
pathogens and greatly increasing the laboratories that study them while
it suggested that “administrative impediments” to GOF research be
removed in its June 2023 treaty draft. This is a way to incentivize lab accidents and leaks.
We urge solutions which ensure both speed in reporting and sharing pathogens,
and in access – in every country – to sufficient tools like tests and
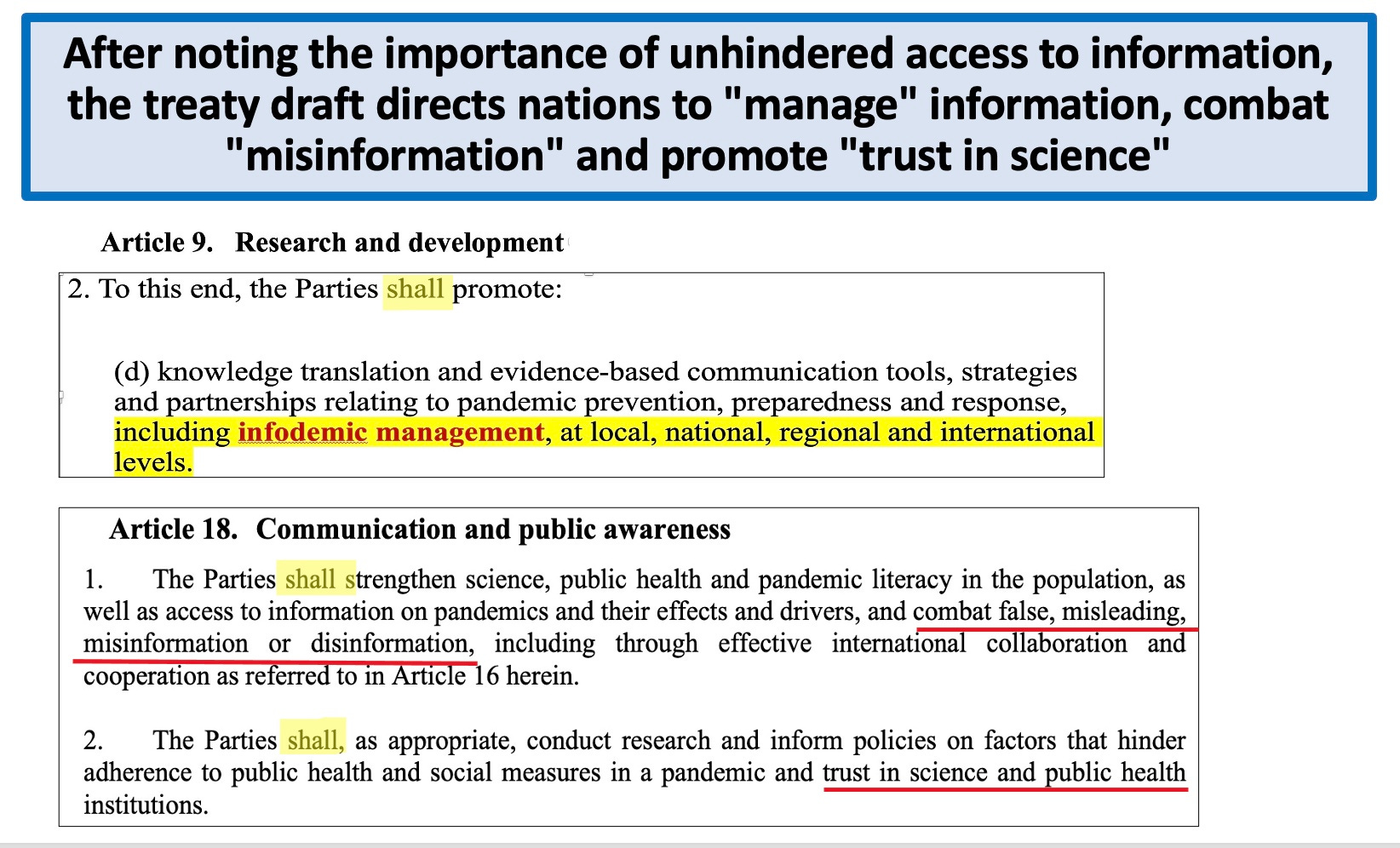
vaccines to protect lives and minimise harm. The public and private
sectors must work together towards the public good. This global effort
is being threatened by misinformation and disinformation. Among the falsehoods circulating are allegations that the WHO intends to monitor people’s movements through digital passports;— Then why did the WHO take over the digital health passports obtained by the EU last June
and start rolling them out already? Is it the monitoring of movements
or the monitoring of finances and vaccine/health data the WHO wants to
obtain? Maybe the “monitoring peoples’ movements” claim is a red
herring to conceal the other monitoring going on?
that it will take away the national sovereignty of countries;—which
it will of course do when the WHO can give orders to nations, require
nations to pass laws to enact the WHO’s directives, and the WHO can
commandeer supplies in one country and move them to another. But don’t
take my word for it. Here is the evidence:
David Bell
and Van Dinh explored this issue in depth. Their article is titled, "
Why Does the WHO Make False Claims Regarding Proposals to Seize States’
Sovereignty?"
https://brownstone.org/articles/why-does-the-who-make-false-claims-regarding-proposals-to-seize-states-sovereignty/
and that it will have the ability to deploy armed troops to enforce mandatory vaccinations and lockdowns.—More
straw man arguments, like the “monitoring movements” argument above.
Straw man arguments create a false assertion so the person doing the
arguing can effectively argue against it, when the person is unable to
argue against the actual proposal in play. No one said the WHO has its
own troops and will use them. It doesn’t. But nations do have armies
and police, and they were used during
COVID to impose lockdowns and in some nations mandatory vaccinations.
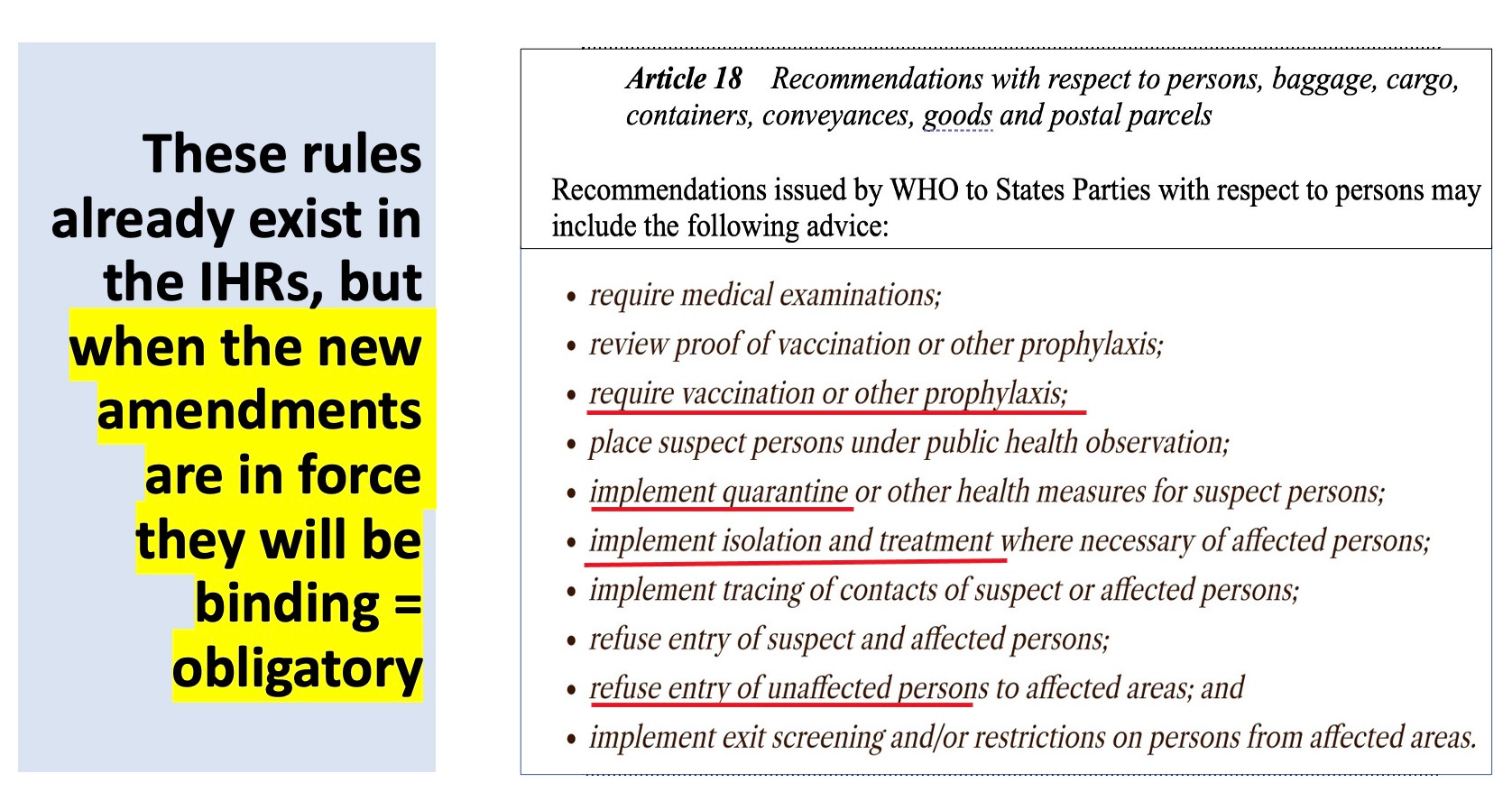
The nations are being told they must obey the WHO, and the WHO is giving
itself the right, in the IHR amendments, to impose lockdowns and
mandatory vaccinations.
All of these claims are wholly false and governments must work to disavow them with clear facts.—I just provided you the clear facts, flunkies.
It
is imperative now to build an effective, multisectoral and multilateral
approach to pandemic prevention, preparedness, and response marked by a
spirit of openness and inclusiveness. In doing so we can send a message
that even in this fractured and fragmented world, cross-border
co-operation can deliver global solutions to global problems.— These virtuosos
write in a way that is not understandable (what do they mean by
multisectoral and multilateral approach to PPPR? What do they mean by a
spirit of openness and inclusiveness?) and the use of flowery language
makes it appear as if they are saying something noble, when the opposite
is true.
We call on leaders of all countries to step up their efforts and secure an effective pandemic accord by May. A new pandemic threat will emerge – except
the idea of pandemic threats, if you remove COVID and HIV, is generally
a fantasy. Less than 1000 people per year have been dying from
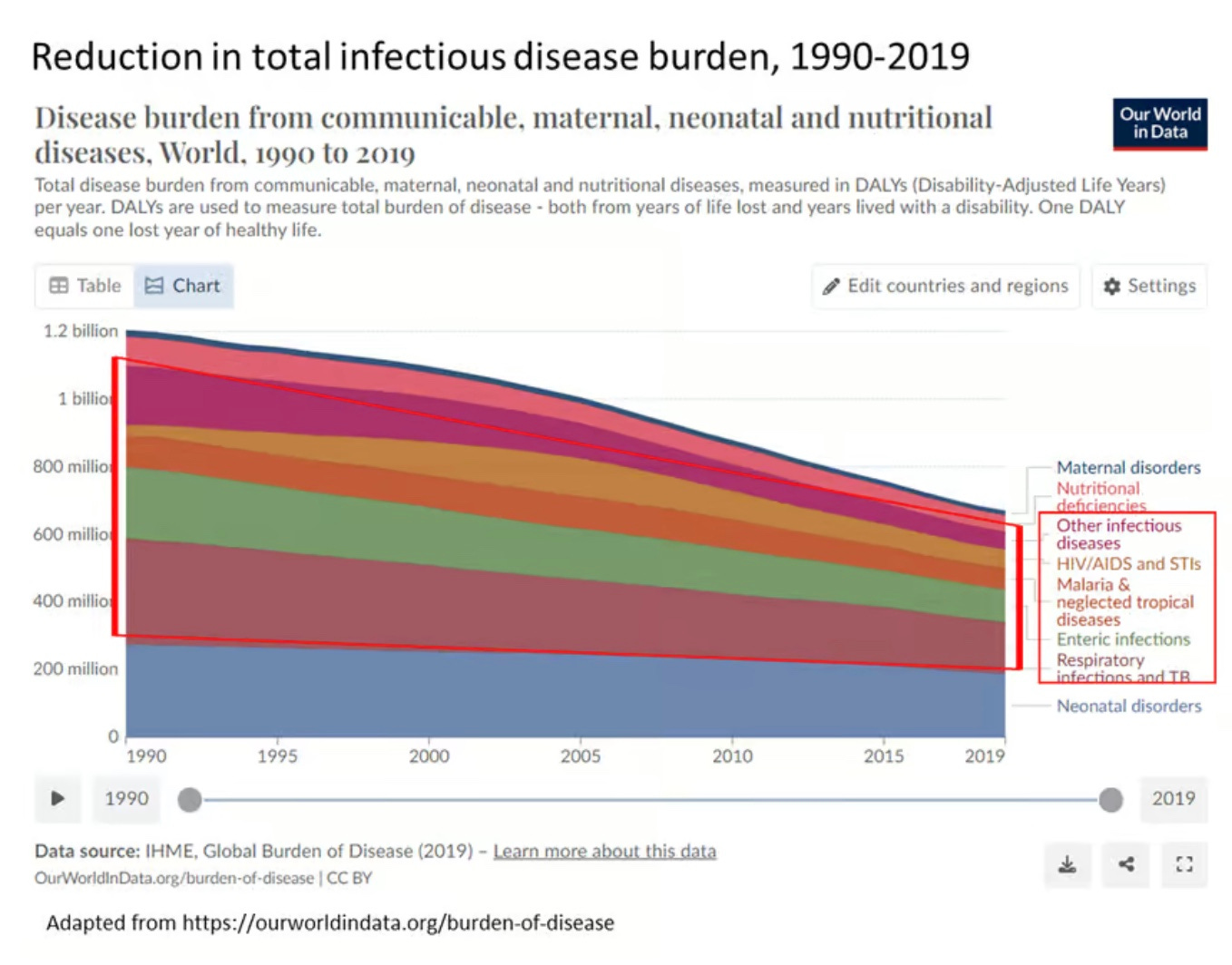
pandemics, despite the fear-mongering. As David Bell notes,
“Generating the fear and compliance necessary to build this new and somewhat parasitic
model of public health has been no mean feat. For decades, life
expectancies have been rising globally while infectious disease deaths
have plummeted.”
https://brownstone.org/articles/the-fairy-tale-of-pandemic-risk/
and there is no excuse not to be ready for it.—Again,
pray tell, how will we be ready by signing this blank check for $41
billion/year to the WHO? How much is each signer of this letter
getting?
We have been scammed on a scale never contemplated. We have to wake up before we are pushed off the cliff.